







Home » Breast Reconstruction
Breast Reconstruction
Conveniently located to serve the areas of Beverly Hills, West Hollywood, Los Angeles and Pasadena, CA
Optimize the natural feel, shape, and symmetry of your reconstructed breast: A sub-specialty in my training as a plastic surgeon and that of my practice is breast reconstruction. Because I am experienced in the complex field of microsurgery, I am able to perform intricate reconstructive surgeries that optimize the natural feel, shape, and symmetry

Of the reconstructed breast as well as minimize the donor site deformity. There are several options available for reconstructing a breast, such as the autologous method, which uses your own natural tissue.
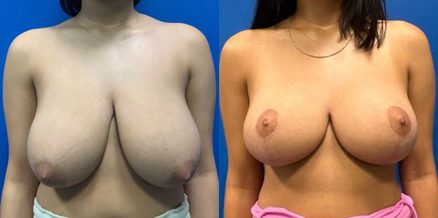
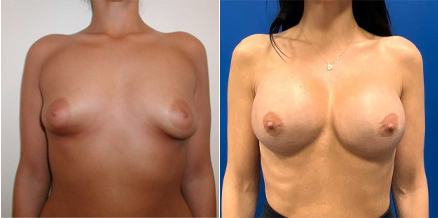
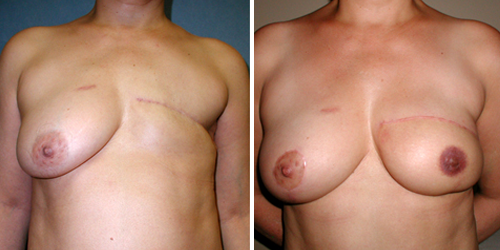
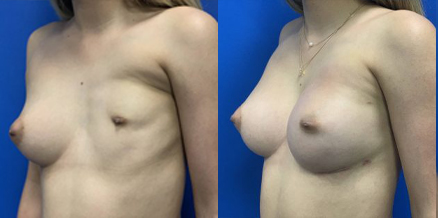
Before and After Photos






Contents
There are several options for breast reconstruction. Selection will be based on medical and oncological criteria as well as the patient’s personal and aesthetic needs. Breast reconstruction is one of the most rewarding procedures I perform as a plastic surgeon. Restoring a breast that has been removed due to cancer or another deformity brings about an amazing transformation for the patient, not just physically but also emotionally as it positively affects their relationships with their loved ones.
Breast cancer reconstruction is an integral component of the multidisciplinary team of doctors and other health care specialists in the care of the patient with breast cancer. At each of the hospitals where I have privileges, these specialists include the Medical Oncologist, Surgical Oncologist, Surgical Pathologist, Radiation Oncologist, Breast Imaging Radiologist, Internist, Nutritionist, Physical and
A breast augmentation with lift is a combination procedure that simultaneously elevates and increases the size of the breasts. Breast lift techniques can address loose skin, downward-pointing nipples and areolas, asymmetry, and other cosmetic issues related to shape. Most of all, the lift portion of the procedure elevates the breasts to counteract the effects of gravity, providing long-term and much-needed support for this transformative improvement. Patients can choose between a variety of implant sizes to achieve the most natural-looking results that flatter their overall body contour.
Single Stage Breast Implant Reconstruction:
The current advent of community outreach and public education about breast cancer and the importance of early detection as well as the findings of certain key genes and gene combinations that predispose patients to have breast cancer have allowed oncological surgeons to safely remove the breast yet spare the breast skin envelope and oftentimes the nipple-areolar complex such that breast reconstruction can be done in a single stage with the use of specific breast implants. At the time of the total mastectomy that leaves the nipple and areolar complex intact, the breast is reconstructed by placing the permanent implant at the time of the mastectomy. The patient who is indeed a good candidate for this type of reconstruction then will be spared the process of tissue expansion and the second stage of exchanging the tissue expander to a permanent implant. It will save one additional trip to the operating room as well as the further steps in creating the nipple-areolar complex and tattooing as the nipple and areola are spared.
Patient selection is key however in making the right decision to undergo this procedure. The first and foremost in the decision making is the oncological safety in sparing the nipple and areolar complex when the breast is recommended to be removed and next is the tissue (skin) integrity and breast shape, contour symmetry, and appearance. All of these details are carefully discussed during a patient’s thorough consultation and in partnership with the oncological breast surgeon to make sure that the patient is indeed a good candidate to have this type of same time implant reconstruction. The final cosmetic outcome appears not unlike a cosmetic breast augmentation as the incision on the breast is the same as in a cosmetic breast augmentation; either along the lower edge of the areola or along the breast fold. The patient, therefore, wakes up after surgery with a new set of breasts that look like and sometimes look better than their original breasts; as they are slightly uplifted, or if there was breast volume asymmetry, it is corrected at the same time as the mastectomy.
The role of an ADM (acellular dermal matrix) and its proper use is key to the successful single stage implant breast reconstruction. The ADM is fashioned to act as an internal brasserie or like a hammock, it supports the implant along its lower half as the chest muscle does not naturally extend to cover the lower half of the breast implant. The use of an ADM has allowed plastic surgeons to reconstruct the breast after mastectomy in a single stage and allow the reconstruction with an implant to have favorable longevity. The ADM becomes incorporated into the skin envelope of the patient and permanently becomes a natural part of the patient’s anatomy. Sometimes minor revisions are done to perfect an initial single stage reconstruction. Almost all revisions if scheduled in patients with single stage breast reconstruction are as out-patient with minimal downtimes and a quick recovery.
Autologous Breast Reconstruction:
This method uses your own fatty tissue and skin from the lower abdomen without the need for an implant and with an added benefit of a full tummy tuck. When a patient qualifies to have the muscle-sparing free TRAM flap the lower abdominal fat and skin are used and transferred to the chest area and shaped into a new breast.
Unlike most TRAM flap reconstructions; this operation does not remove the whole length of the muscle but only a small portion where the blood supply to the overlying fatty tissue and skin is present. This area of the lower abdominal fat and skin is then transferred with the use of microsurgery to the chest area and shaped into a breast. This optimizes the circulation to the newly reconstructed breast, while minimizing the amount of muscle removed from the abdomen which minimizes the chances of a future abdominal wall muscle weakness or bulging. The free TRAM technique is specially used in younger, physically active patients and those who need bilateral breast reconstruction.
Due to this better blood supply, the flap that is transferred to the chest can be shaped and contoured to best match the opposite breast. The newly reconstructed breast often has a more youthful or uplifted appearance such that many women request a lift of the opposite breast. Surgical procedures on the non-cancerous breast to establish a better symmetry with the reconstructed one are considered medically necessary and reimbursable by both commercial and government insurance plans. The common symmetrizing procedures include insertion of breast implants, breast lifts, or reductions.
Latissimus Dorsi Muscle Flap and Breast Implant Reconstruction:
In this procedure, the breast is reconstructed using tissue from the back along with an implant. An example of this would be the latissimus dorsi muscle flap procedure. There are several variations to the skin paddle shape and size and the location of the final incision on one’s back depends on personal preference and the extent of tissue required for coverage. The procedure can be done as a unilateral reconstruction or as a bilateral breast reconstruction.
The reconstruction is based on the robust blood supply to the latissimus muscle and its overlying skin as it can be transposed from the back to the chest area. It is used when the abdomen is not available for a TRAM flap reconstruction, the patient is thin, or when a large amount of breast skin is removed due to the cancer being close to the skin, or if there are significant radiation burns to the skin. The procedure can be done at the same time as the mastectomy or in a delayed fashion.
Staged Tissue Expander to Implant Breast Reconstruction:
A two stage procedure is used to reconstruct the breast with implants. First, a tissue expander is inserted underneath the muscles of the chest after the mastectomy. The pectoralis muscle is elevated and a piece of human ADM is used to span the gap between the lower edge of the elevated pectoral muscle and the chest wall so that the expansion is done more comfortably. In the ensuing weeks to months, this device is slowly expanded as the body learns to accommodate the expander and the chest tissues stretch and begin to relax in preparation for the second stage of the procedure.
After a waiting period of six to twelve weeks, the patient is brought back to the operating room for the second stage when the expander is removed and replaced with an implant. The final implant can be saline or silicone gel.
Reconstruction of Nipple and Areolar Complex:
A second stage for the autologous tissue breast reconstruction techniques described above and as a third stage in the expander/implant reconstruction is the creation of nipple and areolar complex. This is done as an outpatient procedure with minimal discomfort.
Tattooing of the Nipple and Areola:
The final stage in breast cancer reconstruction is the tattooing of the nipple and areolar complex. The tattoo color is chosen to match the opposite breast or in the case of bilateral reconstruction, the color is usually chosen by the patient to mimic her original nipple color.
Contact